RIFE
CANCER THERAPY: APPENDIX B
THE INTENSITY OF ULTRA SOUND
GENERATED IN THE UPPER SURFACE OF THE SKIN BY
THE RIFE FREQUENCY INSTRUMENT
WHICH WILL KILL A CANCER TUMOR
By Physicist Gary Wade
(This is a REVISED and CORRECTED version (
for less technical
article RIFE THERAPY SIMPLIFIED)
There are
now four types of Rife frequency instruments. The original type used an X - ray
tube that had been back filled with helium and or argon gas at low pressure.
This ray tube was used to emit high frequency high intensity light pulses. The
tube also produced direct ultrasound in the room air from the vibration of the
tube walls do to plasma shock waves generated inside the tube. Furthermore,
this tube produced multipole oscillating electric
fields which caused ions in the patients body to
oscillate back and forth generating low intensity ultrasound. The second type
uses electrode contact with the skin to induce a sonic transducer action in the
dead skin layer, induce charge density waves in the body's electrolytic
solution, and produce very low intensity pressure square waves due to constant
drift velocity collisions of the body's salt ions under the influence of the
square wave voltage used. The charge density waves couple with the dipole layer
of charge on the cell membranes to produce broad band ultrasound. This second
type of Rife frequency instrument was popularized by John Crane and will be
discussed in APPENDIX C. The third type uses gas filled tubes at low pressure
as contact electrodes to the body. These gas discharge tubes are supplied with
oscillating high voltages, which produce strong charge density waves in the
body salt solution, high intensity sonic pings in both the tube wall and the
dead skin layer, and low intensity pressure waves in body fluids do to ion
current flow collisions with other molecules. All of these effects cause the
generation of low intensity broad band ultrasound among other things. The
fourth type uses a piezoelectric transducer element which converts voltage wave
forms applied to the transducer into mechanical oscillations that, like the
other types of Rife frequency instruments, destroy the microbe when the
produced mechanical oscillation frequency matches the microbe's lethal
mechanical oscillation frequency.
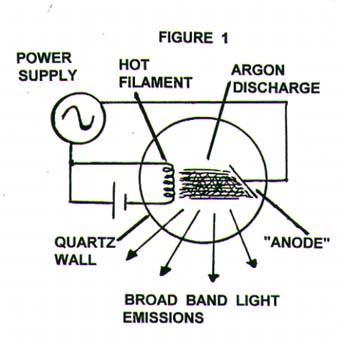
Apparently
on a hunch Dr. Royal Raymond Rife came up with the idea of an audio to radio
frequency intensity modulated gas discharge source for destroying microbes. He
called this device a frequency instrument. It apparently consisted of two
oscillators. One a precision controlled sine or square wave oscillator which
supplied the driving voltage and current to a gas filled tube. The tube was a X-ray tube which had been back filled with helium and or
argon gas to a low pressure. The second oscillator was of a lower frequency and
was probably a square wave oscillator used to turn on and off (modulate) the
higher frequency being supplied to the X - ray tube. This X - ray tube had a
hot tungsten cathode which gave the tube some diode characteristics. That is a
preference for current flow in only one direction. However, do to the high
operating voltages used at low gas pressure along with the ample ion / electron
generation from ultraviolet light emissions from metastable
inert gases used, the tube gas was quite electrically
conductive in both directions. Figure 1 shows a
qualitative diagram of the frequency instrument.
{kind=link}
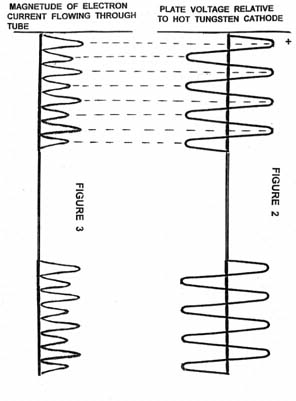
Figure 2 shows a amplitude modulated sine wave voltage being chosen for the
driving voltage for the tube. Figure 3 shows the
magnitude of electron current flow through the "diode" generated by
the voltage signal from the oscillator. The current flows in both directions,
but there is a preferred direction do to the ability of the hot cathode to
easily supply electrons when it is negatively charged relative to the plate
(anode). Note that the current flow is not proportional to the voltage. This is
for two reasons. First, the electron emission from the hot cathode is not a
linear function of plate-cathode potential difference (
voltage ). Figure
4 illustrates how electron emission current depends on plate voltage and
filament temperature. Secondly, the electrons gain kinetic energy on the way to
the anode and if the tube driving voltage is high enough (
and it is ) the electrons gain enough energy to be able to ionize one or
more helium / argon atoms during collisions with them while transiting the ray
tube. These freed electrons join in the current flow across the tube and also
make collisions freeing more electrons. The light emission rate from the tube
which determines the light intensity is proportional to electron collision rate
with helium / argon atoms. The electron collision rate with helium / argon
atoms at a constant tube voltage is approximately proportional to the electron
current. Therefore we should expect the light output intensity of the ray tube
to have the same shape as the electron current magnitude of Figure 3. Also, note
that the X - ray tube wall was of fussed quartz and therefore passed
ultraviolet, visible, and upper end IR "light".
{kind=link}
{kind=link}
Rife
discovered that when he would observe a microbe ( be
it a bacteria, rickettsia, virus or protozoa ) under
his microscope while exposing that particular microbe to a particular discharge
pulse rate from the frequency instrument the microbe would be deactivated. He
found that all microbes had their own specific discharge pulse rate ( frequency ) which deactivated them. Rife called these
their mortal oscillation rate (MOR). Remember, the tube is also producing
direct ultrasound into the air that has the same main frequency as the flashing
light rate. Note that there are two light pulses per single complete voltage
oscillation cycle. In other words there is a frequency doubling effect here.
Rife suspected that some sort of mechanical resonance phenomena in the
microbe's structure was at work in this deactivation process. However, he
apparently did not have any specifics about what the process was. Depending on
the output light intensity and the direct tube wall ultrasound output of the
frequency instrument when operated at the MOR for a particular microbe, the
microbe's reaction could vary from just loosing its characteristic florescent
or luminescent color (as seen in the field of view of the Rife microscope ) to
the microbe violently exploding. Rife found that when test animals which were
infected with a disease causing microbe were treated by the frequency
instrument operated at the MOR of that microbe, the test animals were cured.
Under the
auspices of the Special Medical Research Committee of the
In
Appendix D (on Articles page), the details of how and why specific frequencies
of very low intensity ultrasound can destroy viruses and bacteria are derived
and discussed using standard physics. Here we wish to know the approximate
intensity of ultrasound necessary to kill the cancer virus as was done by the
Rife frequency instrument used in the U.S.C 1934 clinical trials. We should
anticipate three significant physical processes being involved in generating
ultrasound in the patients. One, pressure waves being generated in the patient
from exposure to oscillating light intensity from the X - ray tube. Two, direct
generation of ultrasound from the X - ray tube walls vibrating from their
interaction with plasma shock waves generated by tube electric current flows
and electric fields from oscillating charge density distributions. Third,
oscillating forces on the ions in the salt solution of the patient's body from
the oscillating electric fields of the discharge tube ( X
- ray tube ). These oscillating ions insidee the patient produce pressure waves
(ultrasound).
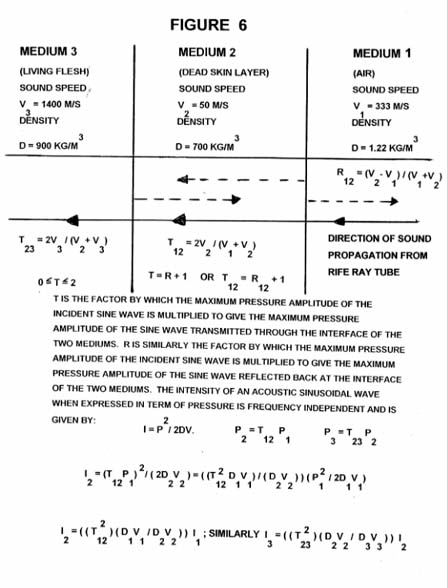
The
intensity (
I = ( P )2
/ ( 2D V ) ; where I is intensity in watts / meter squared , P is the maximum
pressure in Newton / meter squared , D is the density of the medium in
kilograms / meter cubed , and V is the velocity of sound in meters / second in
the medium. P will now be calculated approximately and along with approximate
assumed values for D and V, I will be given to within two orders of magnitude.
With perhaps two orders of magnitude of slop, this may seem like a non-useful
result. However, we shall find that the results have some profound
implications. Figure 6
shows a frequency instrument being used on a cancer patient. Assume the light
leaves the ray tube uniformly in all directions. Then the light intensity on
the patient's abdomen directly below the tube as illustrated in Figure 6b is equal to
the total light out put in watts divided by the surface area of a sphere which
has a radius equal to the shortest distance between the center of the ray tube
and the patients skin surface. We will assume 40 %
efficiency in conversion of electric power to light,
this includes UV, visible, and IR in the ray tube. The quartz wall of the X -
ray tube passed UV, visible and much IR light through it. The tubes used in the
clinical trials dissipated around 80 watts. Therefore, we assume approximately
32 watts of radiant light energy is emitted. Now looking back at Figure 3 we see that
the light is emitted in pulses which to a first approximation can be
approximated as of a sine wave pattern. The 32 watt light output power is the
root mean square ( RMS ) value of the output power in
the form of light. For a sine wave the relationship between the peak power
output and the root mean square value is :
{kind=link}
W ( peak value ) = ( 2) W ( RMS value ). Light carries
momentum and when light is absorbed by the skin, that momentum must be
conserved.
It is
conserved by being converted into the longitudinal wave momentum of the
pressure pulse that travels into the body. The peak amplitude of that pressure
pulse associated with each light pulse is:
P = ( Pointing's vector ) /( speed of
light ) = S / C ; where S is the magnitude of
Pointing's vector and C is the speed of light. S = ( (2) W( RMS value ) ) / ( Surface area of sphere )
S = the
instantaneous energy per time crossing unit area.
P ( peak value ) = ( (2) (32 watts)/(4 )(.3 meters)2 )
/ ( 3 x 10 8 meters/second )
P ( peak value ) = 1.88 x 10 -7 Newton/meter squared
The outer
surface of the skin is made up of a dead skin cell layer. These cells have
approximately 10% water content and the rest is essentially protein. I know of
no density or speed of sound measurements for this dead skin material. I will
now assume a density of .8x10 3 kilograms/meter cubed ( 80%
of that of water ) and a speed of sound of
50 meters
/ second ( similar to vulcanized rubber ). Using these
values for
P ( peak value ), D ,and V we obtain:
I = ( 1.88 x 10 -7 n/m ) 2 / ( (2)(.8x10 3 kgm/m3 )( 50 m/s ) )
= 4.4 x 10 -16 w/m2
It should
be noted that in this approximation calculation, the fact that significant
radiant "light" passes through the dead skin layer and is absorbed in
the living tissue is ignored. Proper consideration of this fact does not
significantly change the results for the value of I calculated.
If the
above calculated value of ultrasound intensity is responsible for a significant
amount of the observed microbe kill off with a Rife frequency instrument, then
there are two important points to be made and realized at this time. First,
even if our approximation calculation for I were off
by two orders of magnitude, it is clear that what is normally thought of as a
totally harmless and insignificant ultrasound intensity can have profound
effects on microbes. We can make this statement because Rife and medical
doctors which used his frequency instrument cured thousands of patients of microbe/virus
caused diseases using power levels in the ray tube we used for calculation
purposes above. The second point to be made is that the microbes and viruses
have high Q-values when considered as mechanical resonators. Where 2E /Q is the approximate total vibration energy released or
dissipated by a vibrating system per complete oscillation cycle of the system.
E is the total energy stored in the oscillator ( potential
plus kinetic energy). This Q-value as used above is understood for a simple
oscillating system, such as a mass attached to a spring while going back and
forth (oscillating ) on a frictional surface. However, in our virus system it
becomes a little more tricky to use, because there are
so many vibration modes that can be simultaneously in existence. For example
when you pick up one of the virus models you have constructed from the material
you have been supplied in APPENDIX D, keep your finger on one of the spherical
protein clumps. Now count to see how many different closed "rings" of
protein clumps this one protein clump belongs to. Note that for each separate
closed ring this protein clump has three independent degrees of vibration
associated with each resonant frequency mode for each closed ring. These three
independent degrees of vibration consist of two transverse vibrations at right
angles to each other and one longitudinal The physical displacement of one
transverse vibration occurs approximately in the local tangent plane to the
surface in which the clump is located and at right angle to the Ring's local
curvature. The other transverse vibration has its displacement occur at right
angles to the first and occurs in the approximate direction of above and below
the local tangent plane to the virus's surface. The longitudinal vibrational displacement occurs back and forth along and
parallel with the local direction of the closed ring of clumped proteins. Once
you realize that all of these vibration modes are allowed to coexist together
on the outer coat of the virus, you see that the coat is a sitting duck, just
waiting to absorb resonant vibration energy up to the point where it comes
apart by rupture of the weak bonding between adjacent protein clumps.
Now, let
us consider the ultrasound intensity generated in the air by the mechanical oscillations
of the wall of the X - ray tube. From the operation of current gas filled tubes
which are similar to Rife's tube, with similar
electrode design, gas mixtures, pressures and power dissipation, it is
experimentally known that such tubes when operated at auditory frequencies make
an audible sound. This sound occurs whether the tube is ran
at mega hertz frequencies with audio frequency amplitude modulation or simply
by a audio frequency sine wave voltage. The sound is not very loud but is
clearly audible as long as the back ground sound is not to
loud. The average human ear can just detect (hear) a tone of ~ 1,000 cycles per
second in a very quite background, at around an intensity level of 10 - 12 W /
m 2. I believe that it is safe to assume ultrasound intensities of around 10 -
10 W / m2 for these Rife type tubes. As stated above the intensity of an
acoustic sinusoidal wave when expressed in terms of pressure is frequency
independent and is given by:
I = ( P ) 2 / ( 2DV); solving for P we have: P = ( 2DVI ) 1/2;
if we now place into this
equation the values of I = 10 -10 W/m2, V = 333 m/S (speed of sound in air), and
D = 1.22 kg/m3 ( air density ), we obtain P = 2.9 x 10 - 4 n/m2. This would be
the approximate sinusoidal air pressure variation experienced on the skin
surface by a patient located only a few inches from a Rife type tube making the
auditory sound mentioned above. Now the important question to ask is: What is
the intensity of the sound that travels into the patient's body generated by the
sinusoidal air pressure variation experienced on the skin? The answer is by
using our formula for intensity again and subtituting
in:
P = 2.9 x
10 - 4 n/m; because the wave pressure is approximately conserved, D ~ .8 x10 3 Kgm/ m3 (dead skin layer), V ~ 50 m/S ,
(assumed velocity of sound in dead skin layer), we obtain:
I = 1.05 x
10 - 12 W/m2
Even, if I
am off ( to optimistic ), and I probably am by a couple or so orders of
magnitude for the intensity of mega hertz ultrasound actually generated by the
tube wall, it is clear again that ultrasound intensities that are normally
thought to be totally harmless and insignificant can have profound effects on
microbes.
What about
the affects of oscillating electric fields from the tube generating ultrasound
in the patient. Well from the positive results from the use of such devices as
the Lakhovsky Multiple Wave Oscillator, it is clear
that we can expect similar results from a Rife frequency instrument when in
close proximity to it.
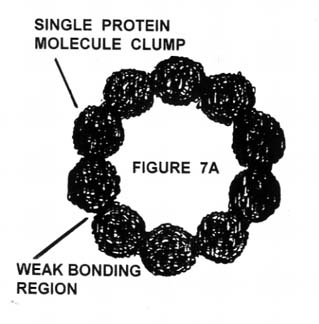
Figure 7a shows a
closed ring of protein clumps such as are found in the outer capsid coat of a virus. Figure 7b shows the
mathematical abstraction of Figure 7a. Each protein clump has a mass m, and
they have a distance a between their centers of mass. The elastic connecting
force is provided by the self elasticity of the protein clumps, which are
weakly bound together mainly with hydrogen bonds. A tension in the closed ring
of protein clumps is maintained by osmotic pressure and, by hydrophilic and
hydrophobic interactions between the outer virus coat and water and other
chemical compounds in the environment ( see APPENDIX D
on Articles page for details. The magnitude of this tension in conjunction with the mass of
the protein clump determines the fundamental natural mechanical oscillation
frequency for the ring.
{kind=link}
{kind=link}
Document 1
is a copy of the actual lab note book used by Rife in his lab on
WARNING,
ultra sound of 11,780,000 cycles per second should not be used to treat cancer
patients unless the required relationship between ultra sound intensity and
treatment time for successful treatment is understood ( see Appendix C for
detail calculations).. From the above approximate calculations Rife probably
used ultra sound intensity of around (10 - 14 w/m2 to 10 - 16 w/m2) for three
minutes once every three days. Usually the patient would be free of all tumors
in seventy to ninety days. What Rife did was to kill off only the surface layer
of the tumor and then allowed the body's immune system to remove the dead
tissue before killing the next layer. All "normal" cancer cells in Rife's time were teeming with either the BX or BY cancer
virus. These cancer viruses are highly absorptive of ultrasound at their
resonance frequencies. Ultrasound at the resonance frequencies is highly
absorbed and exponentially attenuated as it enters a tumor mass. As cancer
viruses in the outer regions ( surface ) absorb
critical resonant vibratory energy they rupture and no longer effectively
absorb resonant ultrasound. The ultrasound effectively penetrates deeper and
deeper into the tumor mass. If the normal ultrasound intensity of around ( 2X 10 4 w/m2) used for physical therapy in sports injuries
is used, all tumors will be mortally wounded within a few seconds. However,
unless serious medical intervention is taken the patient will quit possibly die
in seven to ten days from a combination of kidney failure, liver failure, and
toxemia from the abscess/abscesses formed from the dead tumor mass becoming a
bacterial feeding ground.
It now
seems that bacteria have locations on their cell membrane / cell wall where
they have protein clump type structures similar to viruses in that they form
closed periodically spaced structures. There is enough of the virus coat type
pattern so that there exists at least one closed ring of protein clumps. And of
course this ring can be ruptured by the same mechanisms as the virus form. When
the bacteria's virus like clumped protein structure is ruptured by the exposure
to the acoustic resonance frequency, the osmotic pressure of the bacteria is
relieved by the contents of the bacteria exiting out the rupture site which is
enlarging as the elastic energy of the stretched bacteria cell wall is
relieved. Also, the cell membrane potential difference will collapse. The
bacteria will die.
It should
be noted that the U.S.C. Medical School Special Medical Research Committee that
oversaw the 1934, 1935, and 1937 test trial clinics, which were totally
successful in proving Dr. Rife's cancer cure as well
as the cure of many other diseases never released a report. This committee was
made up of some of the most prominent men in medicine of their time. It is as
though the committee never existed, but they did exist and they did not act
honorably. How many millions of people have died horrible deaths from cancer
and other diseases that Rife had found the cure for? How much money has the
medical industry made on their deaths since the time of the last meeting of the
U.S.C. Medical School Special Medical Research Committee?
For those
people who believe that no medical establishment could be so lacking of
integrity, so lacking of compassion, so dishonor their Hippocratic oath, I suggest you reflect on the
Members of
Special Medical Research Committee of the University of Southern California:
Dr. Milbank Johnson, M.D., member of the board of directors of U.S.C. and
committee chairman, Dr. Rufus B. van Klein Smidt,
president of U.S.C., Dr. Charles Fischer, M.D., of the Children's Hospital in
New York, Dr. Hayland Morrison, M.D., chief surgeon
of the Santa Fe Railway, Dr. George Dock, M.D., of Pasadena, Dr. Karl F. Meyer
of the George Williams Hooper Foundation in San Francisco ( U.C. Berkeley ),
Dr. Alvin G. Ford, M.D., president of the American Association of Pathologists
of Pasadena California.
Other
doctors observing and collaborating on the results of the 1934 U.S.C. Special
Medical Research Committee clinic were: Dr. Ray Lounsberry,
M.D., Dr. James B. Couche, M.D., Dr. E.F.F. Copp, M.D., Dr. Thomas Burger,
M.D., all of the
Taken
from: DR. RIFE AND THE DEATH OF THE CANCER INDUSTRY,
a paper by physicist Gary Wade
P.S. - Two
other much more expanded clinical trials of Dr. Rife's
work were carried out by the U.S.C. Special Medical Research Committee in 1935
and 1937. These clinical trials verified that Dr. Rife had found the cure for
fifty two major diseases. If any institution ever owed the people of the world
a profound apology for its historical corruption, past lack of integrity, past
lack of honor, and past lack of common decency, it is the U.S.C. School of
Medicine. Please feel free to notify the U.S.C. School of Medicine that it is
time for them to reclaim their lost honor by doing the right thing. That is a
prompt, non B.S. program to test out the Rife technology presented in my
various Appendixes. HEY, U.S.C. form an Institutional
Review Board (IRB) to verify Rife technology and quit just training doctors to
be licensed pharmaceutical drug pushers and HMO grunts.
IF YOU FOUND THIS ARTICLE OF REAL VALUE, PLEASE MAKE A HARD COPY WHILE STILL AVAILABLE.
![]()
![]()